
Early Detection
of Heart Defects
Why Screen for Heart Defects?
Congenital heart defects affect 8 out of every 1,000 babies that are born. There are many types of defects, some that create no problems for the newborn, and others that are life-threatening. It is estimated that each year more than 35,000 babies are born with heart problems. The most serious types are called complex heart defects because they require surgery sometimes. Immediately after birth or in the first weeks of life. Because the circulation of the fetus changes immediately after the first breath is taken, complex artifacts must be identified and treated in a timely manner to assure the child has the best possible outcome.
With innovations in surgical techniques, babies born 20 years ago that did not survive, now have a chance of living productive lives. Those born with complex heart defects continue to need special heart care throughout their lives. They may need to pay special attention to how their condition affects issues such as health insurance, employment, birth control and pregnancy, and other health issues. In the in the United States more than 1 million adults are living with congenital heart defects. Since the earlier detection of complex defects results in better care of the newborn and an improved outcome, we provide a screening examination of the heart during each trimester of pregnancy and have the highest detection rate for fetal heart problems in southern California.
Causes of Heart Defects
Well there are risk factor for congenital heart defects, over 90% of heart malformations have no know cause. For this reason, most physicians have classified heart defects as multifactorial, meaning that there is no known explanation for the problem other than the possible interaction between hereditary and environmental factors. For this reason, many physicians have suggested examining all fetuses for heart defects, since most defects arise from pregnancies with no risk factors. The tables list common risk factors for congenital heart defects.
Table Listing Causes of Heart Defects
Maternal Drug Exposure
- Anticonvulsant medication
- Lithium
- Insulin
- Phenylketonuria
Maternal Weight
- Obesity
Maternal Infections
- 1. Rubella
Family History of Congenital Heart Disease
- Previous child: Risk 1 in 20 to 1 in 100
- Previous 2 children: Risk 1 in 20 to 1 in 20
- Mother has CHD: 1 in 5 to 1 in 20
- Father has CHD: 1 in 30
- Advanced maternal age > 35
- Abnormal serum screening for Down syndrome
Chromosomal and Genetic Abnormalities
- Down syndrome
- Trisomy 13 or 18
- Turnor’s syndrome
- Cri-du-chat syndrome
- Wolf-Hirshom syndrome
- DiGeorge syndrome
- Marfan syndrome
- Smith-Lemi-Opitz-syndrome
- Ellis-van Creveld syndrome
- Holt-Oram syndrome
- Noonan syndrome
- Mucopolysaccharidoses
- William’s syndrome
- VACTERL association
1st Trimester Screening for Heart Defects
(12 to 15 Weeks)
-Free-
In 2002, Dr. DeVore wrote an editorial in entitled “First-trimester of Fetal Echocardiography is the Future Now,” in which she reviewed the medical literature and suggested the detection of heart defects was possible as early as 12 weeks of pregnancy. With the introduction of universal first-trimester nuchal translucency screening for Down syndrome, we have had the opportunity to scan thousands of fetuses in the 1st trimester of pregnancy and apply the principles of fetal echocardiography during the time of the NT examination. In a study performed at the Fetal Diagnostic Center we reported detecting complex heart defects at a rate of 4/1000, which is what is expected in the general population at birth. Almost all of the heart defects would not have been detected if we had not examined the heart in great detail using sophisticated ultrasound equipment.
At the present time we are not reimbursed by insurance companies for this type of study and do it FREE OF CHARGE as a commitment to quality care when we perform a “routine” 1st trimester ultrasound examination of the fetus which only requires us to measure the size of the fetus and the nuchal translucency behind the fetal neck.
The ultrasound approach we use consists of high-resolution transducers that include color Doppler of blood entering and leaving the heart. The ultrasound approach includes a transabdominal examination and in many cases an endovaginal examination, which often provides more detailed images of the fetal heart.
Normal Anatomy
This compares the image of the heart when obtained using an abdominal probe and an endovaginal probe. The image using the endovaginal provides more details regarding cardiac anatomy.
This illustrates 4D power Doppler rendering of the cardiovascular system at 12 weeks of pregnancy. This diagnostic tool is used when there is a concern for an identified malformation.
Abnormal Anatomy
13 weeks
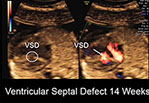
This a clip of a sweep demonstrating findings consistent with coarctation of the aorta as manifest by a larger right ventricle than a left ventricle, a ventricular septal defect and tricuspid regurgitation.
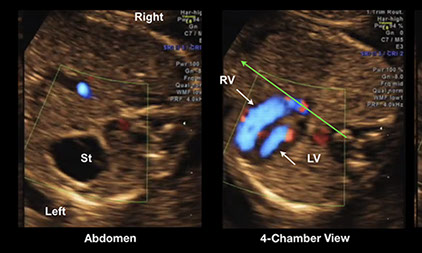
These are images from the above fetus with coarctation of the aorta with the right ventricle (RV) larger than the left ventricle (LV) at 13 weeks of pregnancy. St=stomach,
Normal Anatomy at 13 weeks but Abnormal Anatomy at 17 weeks


the examination of the ventricles at 13 weeks demonstrated the left (LV) and right (RV) ventricles to be of the same size with normal contractility. At 17 weeks the left ventricle was dilated and poorly contracting. This fetus had severe aortic stenosis which developed into a serious heart malformation that would require surgery following birth.







